Dr Choo Wei Chieh tells you why it’s important and what information it should carry.
 Patient empowerment means being engaged with your health and making your own health decisions. In order to do this properly (not to mention safely), one’s health information should be well organised. This means keeping an accurate record of your health such that you can access it whenever necessary, wherever you are, and to share it with whoever necessary (family, healthcare professionals, caregivers, etc.).
Patient empowerment means being engaged with your health and making your own health decisions. In order to do this properly (not to mention safely), one’s health information should be well organised. This means keeping an accurate record of your health such that you can access it whenever necessary, wherever you are, and to share it with whoever necessary (family, healthcare professionals, caregivers, etc.).
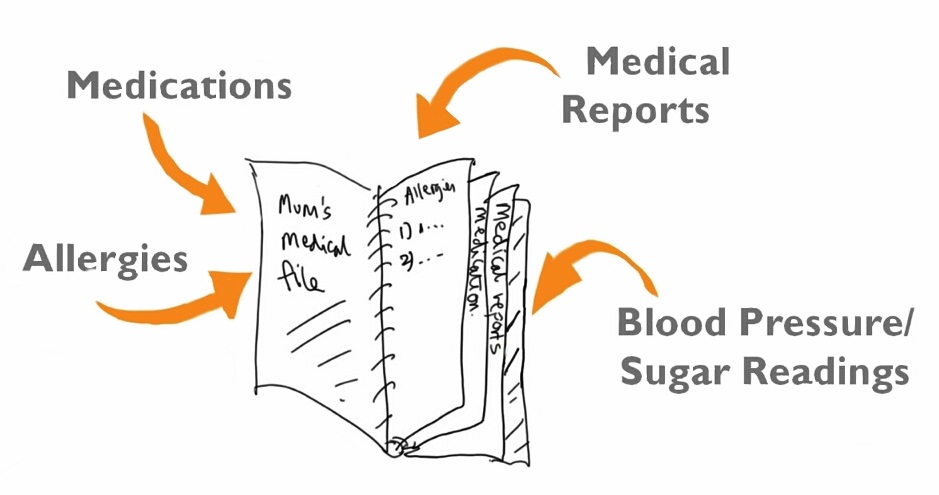
Many patients already keep their medical information organised in files (paper or digital).
- The Personal Health Record (PHR) informs the attending healthcare professional about your medical history.
- It carries your latest health information (hopefully you have kept it updated)
- It ensures continuity of care, especially if you are being cared for by a team of doctors (in different locations) – for eg, a patient with diabetes may suffer from eye and kidney complications, and be seen by an ophthalmologist and renal physician in different offices, who don’t share clinical notes.
- It is a common point of reference for all doctors
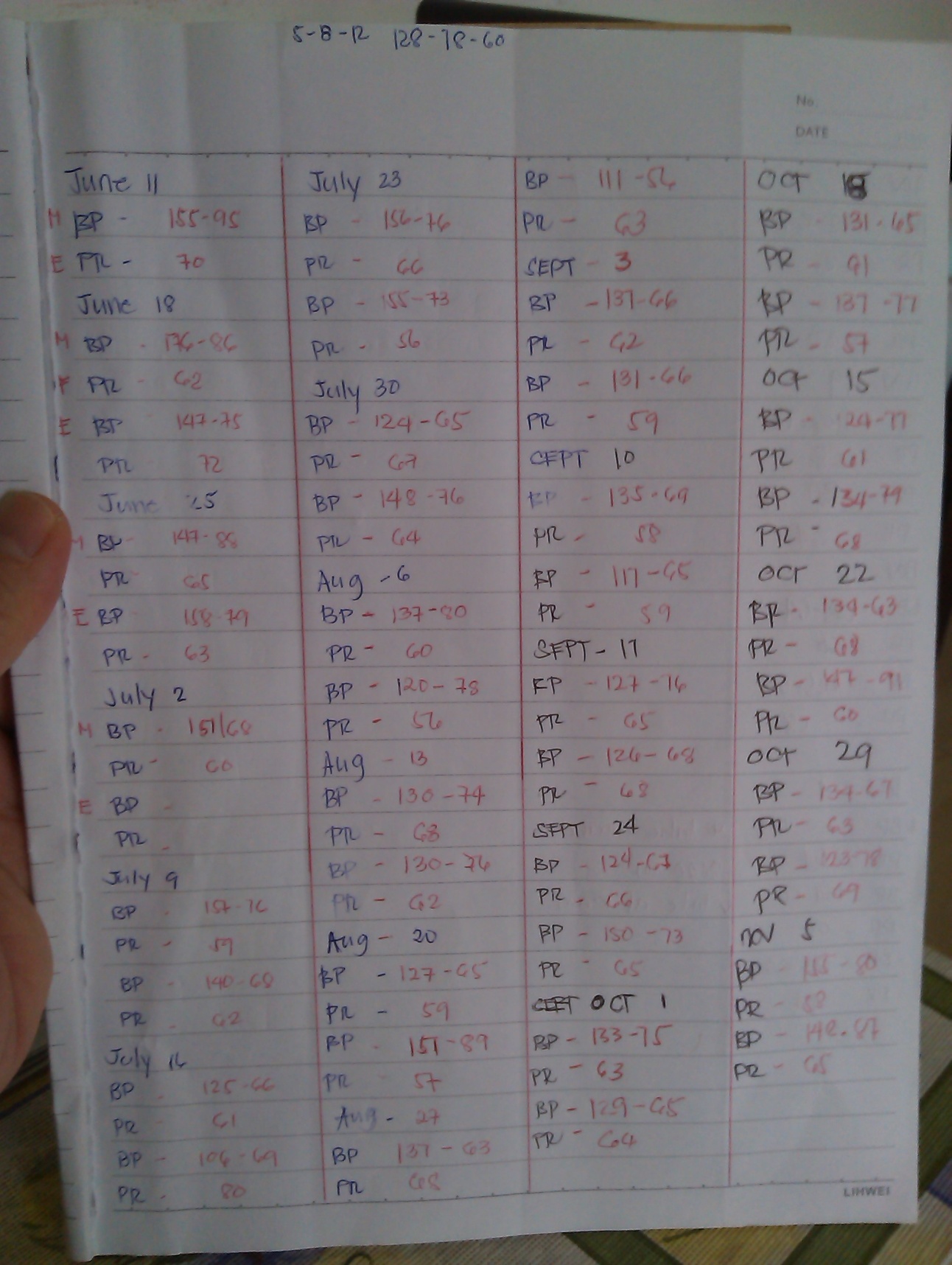
- For patients with chronic disease like diabetes or hypertension, it helps keep track of sugar or blood pressure recordings. Related blood test results and investigations can also be kept to facilitate clinical management.
Your Personal Health Record should hold the following information:
1. Personal information
a. Your name, address, contact number, etc
b. Copies of your Identity documents in case healthcare providers want to see them.
2. Doctors’ contact(s)
a. Situations may arise when your doctors may need to be contacted
by family members of caregivers to discuss your case, get more
information, etc.
b. Include the doctor’s speciality and which aspect of your health he is managing
3. Insurance policies
a. Facilitates claims procedures
4. Allergies
a. Good to include details of incidents leading to allergy
“Penicillin given for sore throat. Led to rash (picture)”
5. Diagnosis
a. List each medical diagnosis (or problem)
b. Brief description if possible
c. Hospital discharge summaries and related investigations
“Stroke leading to right sided paralysis in year 1998. Underwent rehabilitation and therapy with recovery of function in right arm and leg” (attached) CT scan report
6. Medications
a. Include medication name, form, strength, dosage, frequency
“Aspirin (name), tablet (form), 100mg (strength), 1 tablet (dosage), once a day”
7.Health recordings
a. Depending on existing illnesses and medical conditions, here are examples of parameters that patients commonly record:
i. Blood sugars
ii. Blood Pressure
iii. Weigh
iv. Urine volumes
Dr Choo Wei Chieh is the co-founder of IUVO, a mobile-based personal health record system (www.iuvohealthnotes.com).